What is an Audiologist ?
Audiologists are healthcare professionals who provide patient-centered care in the prevention, identification, diagnosis, and evidence-based treatment of hearing, balance, and other auditory disorders for people of all ages. For more information, visit ASHA's Hearing and Balance webpage.
An Audiologist is required to have
- Master’s or Doctoral degree in Audiology
- Minimum of 350 hours of patient care hours obtained in an accredited college or university, in a cooperating program of an accredited college or university, or in another program approved by the board.
- He/she submits to the board evidence that he has passed the examination for licensure to practice
What is a hearing aid dispenser ?
A hearing aid dispenser is someone who is authorized by the state to measure hearing and to fit and sell hearing aids. The credentials for becoming a hearing aid dispenser vary by state, but typically involve working as an apprentice to an already certified dispenser for some period of time and passing a test about hearing aids.A hearing aid dispenser is not an audiologist, and does not have to have a college degree related to hearing loss.
Requirements to become a Hearing Aid Dispenser/dealer
- 18 year old
- good moral character
- free of contagious of infectious disease
- High School diploma or equivalent education (GED)
- pass qualifying examination specified and administered by board
Patients are required to educate themselves regarding the difference between the 2 and the resulting quality of care.
How does the ear work ?
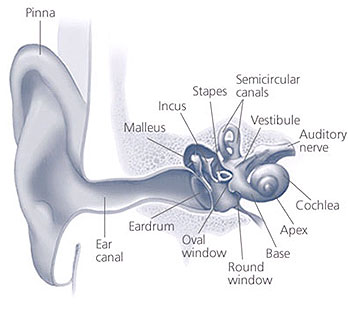 The ear has three main parts:
The ear has three main parts:
- the Outer ear (includes the Pinna and External Auditory Canal),
- Middle ear (Tympanic Membrane and the 3 Ossicles)
- Inner ear (Cochlea)
The outer ear or the Pinna leads into the ear canal (where the wax is formed). The eardrum or the tympanic membrane separates the ear canal from the middle ear. The middle ear contains three small bones which help amplify and transfer sound to the inner ear. These three bones, or ossicles, are called the Malleus, the Incus, and the Stapes (also referred to as the hammer, the anvil, and the stirrup resp.). The inner ear contains the cochlea which changes sound into neurological signals which are conveyed to the brain via the Auditory Nerve.
When sound enters the ear canal, it causes the ear drum to vibrate. As a result of this the three tiny bones (ossicles) move and cause vibrations in the fluid in the cochlea (inner ear). The cochlea is arranged like the keys of a piano and in humans, can hear frequencies as low as 20Hz to as high as 20000Hz. The fluid movement results in the movement of the hair cells in the inner ear converting the mechanical energy into electrical impulses. The electrical impulses are carried by the auditory nerve to the brain and this is where they are interpreted as sound.Types of Hearing Loss
Hearing loss is categorized primarily based on which part/parts of the ear/ears is affected. Hearing loss is most often categorized as Sensorineural, Conductive, or Mixed.Another kind of hearing loss that is not very common is called “Central Hearing Loss” It is also called "central deafness," and results from damage or impairment of the nerves or nuclei of the central nervous system, either in the pathways to the brain or in the brain itself.
"Central auditory processing deficit," is yet another type of loss in which the person has normal hearing, but has difficulty processing and understanding the speech and certain sounds
Styles of Hearing Aid
The following are common hearing aid styles, beginning with the smallest, least visible in the ear. Hearing aid manufacturers keep making smaller hearing aids to meet the demand for a hearing aid that is not very noticeable. However, smaller hearing aids cannot be made powerful enough to give you the necessary loudness that you would need.COMPLETELY-IN-THE-CANAL (CIC) or mini CIC | |
 |
A completely-in-the-canal hearing aid is molded to fit inside your ear canal. It improves mild to moderate hearing loss in adults. A completely-in-the-canal hearing aid:
|
IN-THE-EAR (ITE) | |
 |
An in-the-ear (ITE) hearing aid is custom made in two styles — one that fills most of the bowl-shaped area of your outer ear (full shell) and one that fills only the lower part (half shell). These can be fit on people with mild to severe hearing loss. An in-the-ear hearing aid:
|
BEHIND-THE-EAR (BTE) | |
 |
A behind-the-ear (BTE) hearing aid hooks over the top of your ear and rests behind the ear. A tube connects the hearing aid to a custom earpiece called an ear-mold that fits in your ear canal. This type is appropriate for people of all ages and those with almost any type of hearing loss.
A behind-the-ear hearing aid:
|
RECEIVER-IN-CANAL (RIC) or RECEIVER-IN-THE-EAR (RITE) | |
 |
The receiver-in-canal (RIC) and receiver-in-the-ear (RITE) styles are similar to a behind-the-ear hearing aid with the speaker or receiver in the canal or in the ear. A tiny wire, rather than tubing, connects the pieces.
A receiver-in-canal hearing aid:
|